Bad Breastfeeding Advice We Too Often Follow
This post may contain affiliate links (see full disclosure). As an Amazon Associate, I earn from qualifying purchases.
Are you relying on bad breastfeeding advice without even knowing it? It happens more often than you’d think, and it can leave you wondering where your milk supply went! Here’s what you need to know.
I have spent thousands of hours in breastfeeding support groups online. Breastfeeding isn’t always easy, and in the throes of postpartum life, groups like these can be super helpful. It is awesome to have a support network of people who have gone through–or are going through–what you’re experiencing!
WANT TO PUMP MORE MILK? Try THIS!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
Want to pump more milk? try this!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
But it’s really important to be in a support group run by lactation professionals (like this one I co-run), so you don’t unknowingly rely on bad breastfeeding advice. This advice sounds good, and a lot of breastfeeding parents might even follow it! But if you’re not careful, it can harm your breastfeeding relationshiop.
As an International Board Certified Lactation Consultant (IBCLC), I can tell you what advice to watch out for:

Medical Disclaimer: The content of this blog post is not medical advice nor is it a substitute for medical advice, diagnosis, treatment, or professional lactation care. This post is for educational and informational purposes only. It is the reader’s responsibility to review all information regarding any medical condition or treatment with a healthcare provider.
BAD ADVICE: “TO MAINTAIN SUPPLY, YOU HAVE TO DRINK TONS OF WATER (OR BODY ARMOR, OR WHATEVER IS TRENDING).”
False. Research has actually shown that extra fluids in excess of natural thirst have no effect on milk volume (source)! If you are going to be out in the heat, or if you find that you struggle to remember to drink water (we get busy, it happens), then yes–drink more fluids. But don’t feel like you need to drink some arbitrary number.
The takeaway: Drink to thirst. If you’re never really thirsty, try–as a rule of thumb–having a drink of water every time baby nurses, or drinking until your urine is a very light, pale yellow.

BAD ADVICE: “TO HAVE A GOOD SUPPLY, YOU HAVE TO EAT LACTATION FOODS/DRINKS.”
Cookies. Oatmeal. Fenugreek. Lactation tea. Brewers yeast. Body Armor. Blue Gatorade. Coconut water. The list goes on and on. I’ve even seen someone suggest carrots…??
Here’s the deal. There is virtually NO solid research supporting the efficacy and use of galactagogues (the “official” name for milk supply boosting supplements) (source, source, source).
In fact, fenugreek, an herb commonly recommended for its milk boosting powers, isn’t even recommended anymore in the latest (2018) edition of the Core Curriculum for Interdisciplinary Lactation Care. Fenugreek can make baby gassy and fussy, and can cause upset stomach and gas in the breastfeeding parent. Additionally, fenugreek is actually not recommended for people with diabetes, hypoglycemia, hypothyroidism, people who are on medications to slow blood-clotting, and people who are allergic to peanuts or chickpeas (source).
But I digress.

The fact of the matter is, even a river of blue Gatorade or a mountain of oatmeal will not be enough to increase low supply (if you have it) without also effectively removing milk from the breast an appropriate number of times a day.
The truth is, milk production is about milk removal and nipple stimulation (source). If you don’t have a good latch, or if you aren’t pumping effectively, your supply will be affected.
So while most special lactation drinks/foods–especially non-herbal ones like oatmeal–probably won’t hurt, they are also unlikely to solve the underlying issue. And they tend to distract you from what will really help increase supply: more frequent nursing and/or pumping.
When these galactagogues do “work,” it may be that you needed a calorie boost (which you could have gotten from any calorically dense food). However, it is unlikely that a short-term, small calorie deficit would significantly affect milk volume (source). Experts suspect galactagogues have a strong a placebo effect. Or, it may also be that an accompanying increase in pumping/nursing is what is really doing the trick.
The takeaway: Ensure that baby has a good latch, or that you have a pump that effectively removes milk. Then, remove milk by feeding baby on demand day and night or pumping as often as baby would otherwise nurse.
READ MORE: Why I Don’t Recommend Lactation Cookies & Body Armor For Low Milk Supply
BAD ADVICE: “FEED BABY ON A SCHEDULE, BECAUSE IT’s GOOD FOR them and makes life easier!”
A feeding schedule is a formula feeding norm. And for breastfed babies, it isn’t necessary. In fact, it can even be harmful to milk supply (source, source). And ultimately, if your goal is to breastfeed, worrying about low supply down the road isn’t going to make your life easier.
Babies fed from the breast should be fed on demand in order to maintain milk supply (source). This is a fundamental truth that advocates of “parent-led schedules” miss every time. Breastfed babies do not need to have the time between feeds stretched as they age (this is also a formula feeding norm), and you should question any “experts” who tell you otherwise.

Over time, your baby will fall into a routine. He or she will naturally nap at certain times an eat at certain times. It’s okay to follow baby’s natural routine. But following a parent-led feeding schedule is not likely to help your breastfeeding relationship long-term. In fact, research has shown us that breastfeeding parents who follow parent-led feeding schedules are more likely to stop breastfeeding sooner compared to those who don’t (source, source).
The takeaway: Feed on demand. Routine is fine. Schedule is not. If you find you need to feed on a schedule, consider working with a lactation consultant to develop a plan to protect your milk supply.
READ MORE: Milk Supply Dropping? Your Feeding Schedule May Be Why
BAD ADVICE: “GOT CRACKED, PAINFUL NIPPLES? JUST PUSH THROUGH IT!”
Breastfeeding at first will be uncomfortable. I won’t lie.
But discomfort is different from straight up pain. If your nipples are cracking, bleeding, causing you to gasp or hold your breath or curl your toes–this is not normal. If the discomfort lasts more than a week or two–this is not normal. It is a sign that something is wrong.
Waiting too long to get help can sometimes jeopardize breastfeeding. It’s better to get help right away.
The takeaway: The answer to the problem of nipple pain is not to push through it. It is to get help! Preferably right away, and preferably in person with an IBCLC if possible.

Please Note: Not everyone who calls themselves a “lactation counselor” or “lactation consultant” or “lactation nurse” is an IBCLC. Some providers without this credential are still qualified to assist with latch and painful nipples. But if your problem is not getting better or if you feel the advice you’re getting seems off, do not be afraid to get a second opinion from a different lactation professional! Pediatricians usually do not have lactation training and are therefore usually not the best source of lactation advice.
BAD ADVICE: “JUST USE A NIPPLE SHIELD.”
A nipple shield is a thin piece of silicone that goes over the nipple. Babies with difficulties latching may be able to latch with the assistance of one of these, and they can sometimes provide some relief for sore nipples or help a baby latch and suck. They can be a very useful tool!
However, a nipple shield is not usually the best long-term solution. Ideally, they should be used under the guidance of an IBCLC with a plan in place to wean from it. Unresolved latch issues or nipple pain can cause supply issues down the road or put you at increased risk for plugged ducts and mastitis (source). So you really want to get down to the root of the latch issue.
The takeaway: A nipple shield is primarily a band-aid, and it should be treated as sign that in-person help is needed. Sometimes they can be successfully used long-term.

BAD ADVICE: “DON’T LET THE BABY USE YOU AS A PACIFIER!”
The baby is not using you as a pacifier. In fact, baby is using a pacifier as a YOU! It is not a coincidence that pacifiers are nipple-shaped.
There is literally no research to suggest that comfort nursing causes attachment, development, or sleep issues. It is very difficult to overfeed a breastfed baby, and in fact the opposite it true: research has shown time and again that bottle feeding is what is associated with later childhood obesity (source, source, source)
And besides–comfort is a valid need! We wouldn’t tell adults to forego a hug or a favorite pillow or a midnight snack on the basis that those things are “just” for comfort. So why do we hold babies to a higher standard?
The takeaway: If comfort from a pacifier–or a security blanket or beloved stuffed toy–is totally legitimate, why isn’t comfort from the breast?

BAD ADVICE: “YOUR MILK MIGHT NOT BE FATTY ENOUGH. TRY EATING MORE FAT.”
How your milk separates when it is cooled is ultimately of very little importance. “Foremilk” and “hindmilk” are distinctions of little importance too (source, source).
Research has shown there is nothing you can eat to change the total amount of fat in your milk (source, source). The body doesn’t produce “skim” milk–it produces exactly what baby needs. Milk fat quantity changes depending on the time of day and on how “drained” (the breast is never truly empty) or full the breast is (source).
All human milk is nutritious. Make sure that baby has a good latch, feeds on demand, and is showing signs of appropriate milk intake (weight gain and appropriate diaper output). You can learn more about breastmilk fat (and why you don’t need to stress about increasing it) here.
The takeaway: Weight gain issues in babies are almost never a quality issue (i.e. milk isn’t fatty enough) and are almost always a quantity issue (baby isn’t getting enough milk–usually due to a latch or milk transfer issue).
READ MORE: How To Make Your Breastmilk Fattier (And What Doesn’t Work)

BAD ADVICE: “YOU SHOULD PUMP AFTER FEEDS TO BUILD A STASH. YOU NEED A GOOD SIZED STASH.”
Most breastfeeding parents do not need a whole freezer full of milk. Those who have one are either exclusive pumpers, milk donors, and/or tend to have massive oversupply.
Oversupply seems like a good problem to have, but it can actually be just as problematic as low supply. It puts you at increased risk for clogs and mastitis (source), and it puts baby at risk for painful gas, reflux, and frustrating breast rejection (source).
Many breastfeeding parents recommend collecting “leaked” milk with a Haakaa pump, but this can also cause oversupply and its associated issues, since the Haakaa pump does more than just catch what would otherwise leak during a letdown: It draws out additional milk via suction.

But what about going back to work?
In order to maintain your supply while employed outside the home, you will need to pump at work about as often as baby would otherwise nurse. Relying on a large stash to go back to work–and not pumping as often while there–can make milk supply tank quickly.
The takeaway: Typically–unless you are exclusively pumping, pumping for a missed feed, or needing to supplement pumped milk for medical reasons–there is no need to pump extra to build a large stash. Breastfeeding is designed to maintain supply long-term by itself. Feed your baby, not the freezer, and don’t stress about a huge stash!

BAD ADVICE:“TRY SLEEP TRAINING OR A TOP-OFF BOTTLE TO GET BABY TO SLEEP.”
I have already devoted an entire post to the myth of “good” infant sleep, but did you know that early sleep training (and sometimes any sleep training) is actually associated with low supply?
Babies who aren’t nursing at night when they naturally would are sometimes also not making up for that nursing during the day. And since frequency of milk removal and nipple stimulation helps maintain your milk supply (source), it makes sense that a decrease in these things more often than not result in a decrease in available milk.
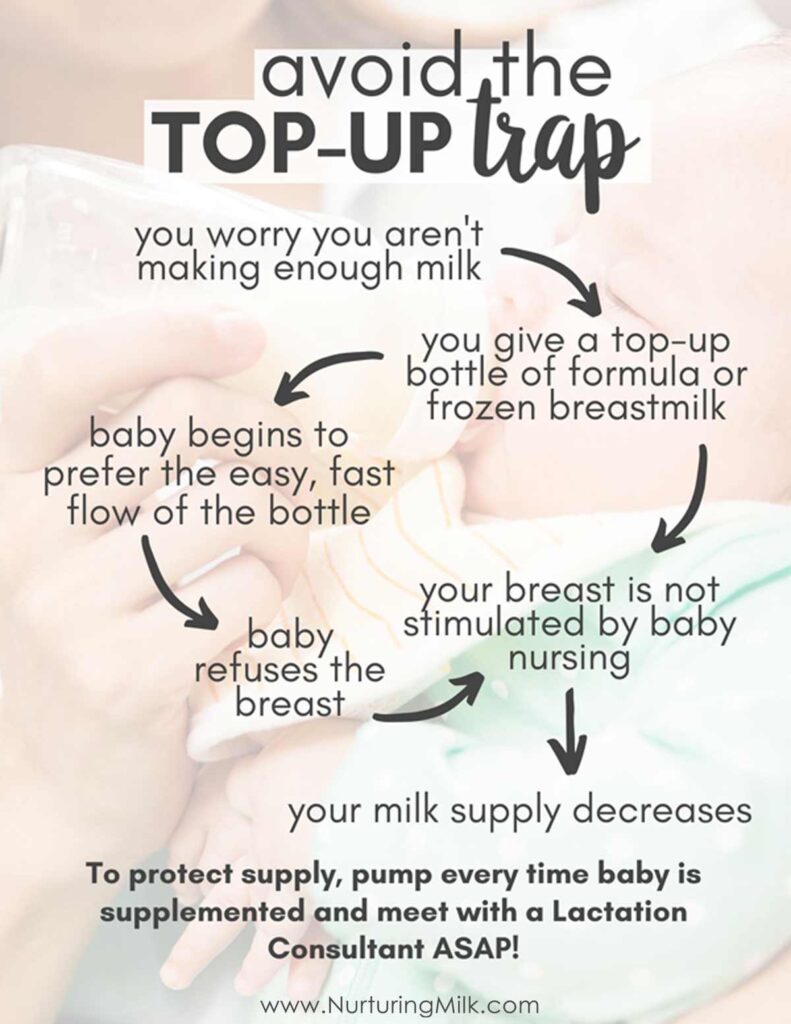
And don’t forget the top-off trap! The body has no way of knowing if baby is getting milk from a bottle, so unless you pump for every bottle of supplement baby gets, you risk a supply decrease. There is no research to suggest a top-off bottle of formula helps babies sleep better (source)–in fact, it may make some babies sleep worse, since formula is harder on the belly (source).
The takeaway: If you are struggling with supply, baby is younger than 6 months, and you are sleep training, consider nursing or pumping at night to help your supply. And fear not: Studies have shown that breastfeeding parents nursing at night often report getting more sleep, not less (source).
NOT ALL BREASTFEEDING ADVICE IS GOOD ADVICE
Lactation is a relatively new field.
“Lactation consultants” weren’t even really a thing until the late ’80s, and lactation training hasn’t been well standardized. It’s not routinely covered thoroughly in medical school, nursing school, or pediatric training programs. And although other parents may have personal experience breastfeeding, their experience might not be applicable to your unique situation!
So it’s important to make sure that the breastfeeding advice you’re getting is evidence-based. Watch out for advice that discourages baby from nursing or promotes parent-directed baby schedules, and don’t be afraid to seek second opinions!
READ MORE: How To Find A Lactation Consultant Who Supports You
Breastfeeding FACTS You Should Know
Our FREE guide will offers 12 breastfeeding secrets to help you avoid common issues.
What no one tells you about breastfeeding (but should)
This is what lactation consultants want you to know. Our FREE guide will give you 12 breastfeeding secrets that will help you avoid common problems.

If you enjoyed this post, be sure to check out our digital library of helpful resources that quickly teach how to avoid common breastfeeding problems and give you the peace of mind and confidence you need to meet your breastfeeding goals.