Everything You Need to Know About Tongue Ties
This post may contain affiliate links (see full disclosure). As an Amazon Associate, I earn from qualifying purchases.
Maybe latching is painful, or baby isn’t gaining weight well despite everything you’re doing to combat low milk supply. Tongue ties and lip ties might be to blame. Here’s how to tell if your baby has a tongue tie, and what you should do about it.
Tongue ties are perhaps one of the most misunderstood and controversial topics in breastfeeding.
When bottle feeding became the cultural norm in the 20th century, we weren’t thinking much about tongue ties. If a baby couldn’t breastfeed or couldn’t breastfeed well, the reason why didn’t matter much, since baby was likely to be given a bottle anyway. But now that breastfeeding rates have been climbing over the last 30 years, tongue ties are trending.
But should they be?
Breastfeeding FACTS You Should Know
Our FREE guide will offers 12 breastfeeding secrets to help you avoid common issues.
What no one tells you about breastfeeding (but should)
This is what lactation consultants want you to know. Our FREE guide will give you 12 breastfeeding secrets that will help you avoid common problems.

Many providers argue that tongue ties are a “fad,” an excuse to make a few extra bucks on an unnecessary procedure. At the same time, others argue that the benefits of releasing a tethered tongue far outweigh any costs. One 2000 study found that 40-77% of pediatricians and ENTs believe that ties rarely cause feeding difficulties, while 69% of lactation consultants believe ties frequently cause feeding difficulties (source). So which is it?
As a lactation consultant myself, my answer will probably be biased. But that bias stems from personal experience breastfeeding tied babies, experience working with parents of tied babies, and learning from colleagues and experts (several of whom are pediatricians, pediatric dentists, and ENTs) who have not only seen thousands of babies, but who have made studying ties their life’s work. Here’s what I’ve found, and what you should know:
Signs and Symptoms of Tongue ties and Lip Ties
Tongue ties and lip ties often play together. If you’ve been told that your baby has a lip tie but no tongue tie, I would encourage you to get a second opinion. According to one expert, the presence of a lip tie indicates the presence of a tongue tie over 90% of the time (source). Which is why some of these symptoms are a result of restrictions in both baby’s tongue and lips.
Here are some of the more common symptoms I often see. Do any of these resonate with you?
Signs and Symptoms in the Breastfeeding Parent
- Sore, “lipstick” shaped, cracked, or bleeding nipples – This tissue damage usually occurs pretty immediately after birth and can range from mild to severe. Severe nipple pain or damage in the first 1-3 days after birth warrants a tie assessment immediately (keep reading to learn how to do this properly). Nipple pain caused by ties rarely goes away on its own and should be addressed. However, not all parents breastfeeding tied babies necessarily experience nipple pain.

- Nipple blanching or vasospasm – This is a type of nipple pain that is caused by reduced blood flow to the nipples, usually as a result of baby’s hard palate clamping down on them (with a deep latch, baby’s soft palate cushions the nipple). Vasospasms feel like shooting breast pain. Blanched nipples will look white when baby unlatches.
- Low milk supply – When a baby is tied, their latch makes it difficult for them to remove milk from the breast well (this is called “poor milk transfer”). Over time, this can cause low milk supply. Because it can sometimes take a few months for this low milk supply to develop, many parents don’t realize the true cause of their low supply.
- Frequent feelings of engorgement – If baby isn’t draining the breasts well, the breasts will often feel full. Sometimes this is mistaken for oversupply. Over time, breasts that aren’t drained well will start to produce less milk.

- Clogged ducts and/or mastitis – Mastitis is a breast infection that can happen as a result of clogged ducts or from pathogens entering the breast. Milk regularly flowing through the breasts helps prevent clogs and mastitis. But tied babies often have difficulty feeding well, so milk is often left sitting in the breast, making it easier for bacteria to take hold and create an infection.
Signs and Symptoms in the Tied Baby
- Shallow or ineffective latch – This latch may or may not be painful. Shallow latch is what usually causes nipple pain and damage, but not always. If the latch is shallow or ineffective, baby will not be able to remove as much milk from the breast.

- Slow weight gain – This is a result of having trouble getting milk from the breast. If you have oversupply or a fast letdown, a tied baby can sometimes get enough milk to gain weight, despite their ineffective latch. However, this oversupply often regulates (as it should) at 3-5 months postpartum, so some tied babies don’t have obvious weight gain issues until then.

- Inability to latch or stay latched – Baby might slide off the breast or might not open wide enough to latch on. Some babies can latch onto the breast with a nipple shield but can’t latch well (or at all) without one. And some severely tied babies might even have difficulty latching onto a bottle.
- Upper lip tucks in– The upper lip should be flanged (like fish lips) or neutral, resting on the breast. If the lip is tucked in, sometimes you can manually untuck the lip and all is well. However, if baby keeps tucking the lip in or you cannot untuck it, this can be a sign of a lip tie.
- Inability to open the mouth wide or a “small mouth” – This is common in tongue tied babies and can contribute to a shallow latch.

- Very strong suck (possible blisters on the lips) or weak suck – When baby can’t stay attached to the breast with a proper latch, sometimes they compensate by sucking very strongly, which can sometimes leave blisters on the lips. Other babies are too tied to suck strongly. These babies with a weak suck are often blamed for being “lazy eaters,” but laziness is never the true cause of a weak suck.
- Clicking and/or milk leaking from the sides of the mouth – Clicking is a “tch tch tch” noise that happens when baby’s lips fail to create a seal on the breast. Sometimes this seal will break if the breastfeeding parent has a fast letdown or oversupply, so clicking doesn’t always indicate a tongue tie and oversupply should be ruled out.

- Spending an excessively long or short time feeding – Some tied babies will do marathon nursing sessions, feeding for an hour or more each time. Others will feed for just a few minutes before becoming exhausted and falling asleep. Given that newborns are known to cluster feed and fall asleep easily, normal newborn behavior should be ruled out.
- Excessive gas and reflux, possibly colic – When babies cannot latch well enough for form a seal around the breast, they can swallow air when they feed, which can result in excessive gas or reflux. Oversupply and dairy intolerance can also cause these, so both should be ruled out.

- Gagging, choking, sputtering on milk or solids – Tongue ties can affect a baby’s ability to coordinate sucking, swallowing and breathing. Older tied babies can have aversions to or difficulties with certain food textures.
- Tooth decay or a gap between the top front teeth – The tongue plays a role in wiping the teeth clean of debris. When the tongue’s range of motion is limited, bacteria can be left sitting on the teeth. Lip ties can create pockets that trap food and bacteria near the front upper teeth. Lip ties can also keep the top front teeth from coming in next to one another.

- Speech delays – Tongue movements are important while speaking. Tied children can have difficulties moving the tongue as needed for proper speech.
- Interrupted sleep or sleep apnea – Tongue ties are often associated with a high palate and mouth breathing while sleeping, both of which can contribute to sleep apnea.

PROPER DIAGNOSIS OF TIES
The frustrating thing about tongue and lip tie symptoms is that they can sometimes mimic symptoms of other issues, such as oversupply and dairy intolerance. Ties also fall on a spectrum, so not all breastfeeding parents and babies will experience all symptoms or experience them to the same degree.
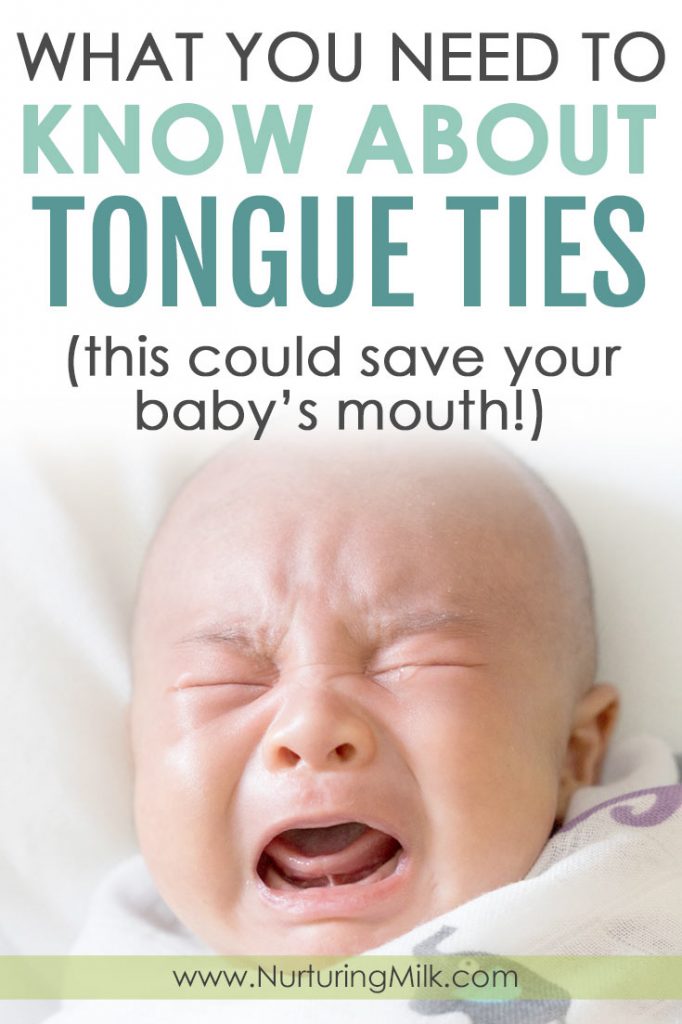
Furthermore, not all tongue ties are visible. Some tongue ties have an obvious stretch of skin connecting the tongue to the floor of the mouth, but not all ties look like this. Some ties are invisible and must be felt for by an experienced provider. As a result, getting a tongue tie properly identified and diagnosed is often very difficult.
It is made even more difficult by the fact that our understanding of ties is relatively new and evolving (we only started to really understand how ties affect breastfeeding in 2008 [source]). Most pediatricians, pediatric dentists, and ENTs have not received the most up-to-date training on tie diagnosis and revision unless they have taken the initiative to seek that knowledge themselves, and very few do this.
For perspective, I live in a metro area of 4.8 million people, and there are only 4-5 providers that I feel comfortable sending a parent to for tie diagnosis and revision. This isn’t because I’m picky: It’s because so few providers in my area have demonstrated a history of properly identifying and revising ties. And this isn’t unique to my area. This is also the experience of thousands and thousands of parents.
Unfortunately, there is a long history of providers inadequately trained in ties diagnosing and revising babies improperly. As a result, the procedure “doesn’t seem to help,” which makes it seem as though the tie wasn’t the problem or the procedure wasn’t necessary. This history is why some providers dismiss ties as a “fad,” and many parents wind up being told their tied babies are just fine.

[Image Credit: DonyaHHI / Shutterstock.com]
My biggest piece of advice to breastfeeding parents who suspect a tongue tie, or who would like to rule one out, is to see a preferred provider for diagnosis and, if needed, revision. (Read that one more time. It’s critically important.)
A preferred provider is someone who comes highly recommended in your area and who has a demonstrated history of properly diagnosing and revising ties. This person is probably not your current pediatrician, pediatric dentist or ENT, nor is this person likely to be the first provider you’re referred to. A preferred provider is usually someone you have to specifically and carefully seek out.
To find a preferred provider, I recommend starting here or joining this Facebook group to ask for recommendations. If that doesn’t work, you can always contact me and I will do my best to assist!

Do Ties Need Treatment?
This is a hard question to answer. The right choice depends on your baby and your breastfeeding goals.
As I’ve said, ties fall on a spectrum. Not every tied baby will have every symptom. Some will have very few. Some babies have some signs of a tongue tie but have absolutely no issues with breastfeeding, while others are so severely tied they cannot even properly bottle feed. While it is true that many tied babies go on to have issues with tooth decay or speech delays, many also do not.
Here are some things you should consider:
1) What are your breastfeeding goals?
If ties are interfering with breastfeeding, do you wish to continue breastfeeding? Are you open to supplementing with pumped milk or formula in a bottle or supplemental nursing system? How do you feel about bottle feeding? If your goal is to provide breastmilk, how do you feel about pumping?

2) How significant are baby’s symptoms? To what degree are you experiencing pain or difficulty?
Some parents and providers will recommend revising all ties in the hopes of avoiding the possibility of future issues. Others are more conservative in their approach, preferring to leave baby’s mouth alone if they feel a revision isn’t clearly or immediately beneficial.
My oldest baby was so significantly tied, she could not stay latched onto my breast by herself. She had very limited range of motion in her tongue and upper lip, and I felt that our odds of future difficulties were very high because of this. We chose to have her revised. My second baby had some minor physiological signs that might indicate a tongue tie, but we had absolutely no issues breastfeeding whatsoever. I felt the odds of future difficulties were very low. We chose to leave her mouth alone. She’s three now and hasn’t had issues.

Deciding to revise can be a difficult decision without a super clear answer. Be sure to speak with your preferred provider about the benefits and risks of a tie release. Some possible risks include:
- Some pain – There are relatively few nerve endings under the tongue and upper lip, and these areas do not bleed very much. Ask your provider what pain relief measures they take and how they recommend you relieve pain after the procedure. Fortunately, there is a lot you can do to very effectively minimize pain.
- Follow up stretches – Stretches of the lip and tongue after the procedure that are designed to prevent the tissues from healing fused together again. Stretches are very important to prevent this reattachment. As a parent, I can say from experience that the stretches made ME feel awful because it looked painful, but my baby often slept through them.
- Risk of oral aversion – Any time you do a procedure in a baby’s mouth, there is a risk that baby will want to avoid breastfeeding or feeding for some time after. This is usually short lived, but can be difficult and frustrating for you and baby.
- The need for follow up care – A tie revision is not always a magic bullet that solves all breastfeeding issues immediately. For some lucky parents, it is. But usually, you will need to follow up with an IBCLC who has experience working with tied babies. Babies often have to re-learn how to use their mouths and feed properly. Some providers recommend therapy to help loosen and release tension in baby’s jaw and face now that the tie is released, and this can be very helpful. This follow up care might be as little as one visit, or it could be beneficial to have baby seen a few times over a few weeks depending on your baby’s needs.

Some possible benefits of a tie release include:
- Improved breastfeeding – Less pain, improved weight gain, and improved milk supply
- Increased likelihood of meeting your breastfeeding goals
- Improvement of other tie symptoms – Reduced gas, reflux, and/or colic
- Reduced risk of future issues – Like speech delays, tooth decay, and sleep apnea
- Improved mental health – For some, not being able to breastfeed may have a negative impact on mental health. I had postpartum anxiety, and the idea of switching to bottles or managing exclusively pumping was extremely overwhelming to me (on the flip side, some may find their mental health improves by switching to bottles).
What Should Your Next Steps Be?
If you suspect a tie, your first step should be to find a preferred provider using the links recommended above. If there are no preferred providers local to you, it might be worth the drive if one is not too far away. If that’s not an option, here are some questions you can ask your provider to get a feel for how experienced they are at treating ties (source):
- How many tie procedures do you perform per month? There is no right answer here. You are mainly trying to get a sense of whether or not the provider views tie releases as a hindrance to breastfeeding that should be resolved. A provider who only releases ties in extreme circumstances may not be someone you want to see.
- Do you treat posterior ties as well? A “posterior” tie is one that is submucosal. In other words, the tongue is tethered to the floor of the mouth, but you aren’t able to see an obvious stretch of tissue under the tongue (called an “anterior” tie). Every tie has an anterior and posterior component, so you want to make sure that the provider doesn’t just release the visible component and leave the invisible one in place, hidden below the mucosa. An experienced provider should know what you mean by this question.
- Do you require general anesthesia? Tongue tie procedures can be safely done without anesthesia (source), and they are done this way all the time. A provider who insists on general anesthesia for all tie releases may be inadequately trained in ties.
- What is your post-procedure stretching routine? If a provider doesn’t have one or says they’re unnecessary, it might mean they are unfamiliar with the concept of reattachment. I would recommend seeking a different tie provider in this case, since this way of thinking often accompanies improper or incomplete tie releases.
Seeing the right provider for tie release is very important. It would be a shame to have to undergo a second procedure because the first was done improperly, incompletely, or because the tissues reattached!

WHAT TO EXPECT
After you’ve found your provider, familiarize yourself with the recommended stretches. One tie expert, Dr. Ghaheri, has a video demonstrating the stretches he recommends, which you can view here.
Expect to do these stretches frequently and diligently in order to avoid reattachment. Dr. Ghaheri recommends that stretches be done 6x a day for the first three weeks, and then during the fourth week, taper off from 6 to 5 to 4 (and so on) down to once per day at the end of the fourth week. Take care to go no more than 6 hours between stretches and do at least one stretching session overnight. This may sound overwhelming, but in practice, it isn’t bad. The stretches don’t take long at all–less than a minute or two.
The wound after a properly done tie release should be a diamond shape, and with appropriate stretching, the wound will continue to look diamond-shaped as it heals.

It is normal for the wound to turn white or a bit yellow several days after the procedure, so don’t be alarmed if you see this. If you are concerned about infection, check with the provider who did the release. You can see what wound healing progression looks like here.
If you need to supplement formula or pumped milk while treating a tongue tie, be sure to pace feed all bottles and protect your milk supply by pumping a full session every time baby gets a bottle. Both of these things are very, very important!
You GOT THIS.
A tie release procedure can feel very overwhelming, especially if you’re already dealing with weight gain or milk supply issues. Know that you are not alone in feeling what you’re feeling! As a breastfeeding parent who was once in the same situation, I deeply empathize.
For us, choosing to revise was the right call. But only you can determine what is the best decision for your family moving forward. Hopefully the information in this blog post will help you make an informed decision.
WANT TO PUMP MORE MILK? Try THIS!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
Want to pump more milk? try this!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
If you enjoyed this post, be sure to check out our digital library of helpful resources that quickly teach how to avoid common breastfeeding problems and give you the peace of mind and confidence you need to meet your breastfeeding goals.