When To Get Breastfeeding Help Right Away (10 Breastfeeding Red Flags)
This post may contain affiliate links (see full disclosure). As an Amazon Associate, I earn from qualifying purchases.
Are you new to breastfeeding? Have other parents told you that an issue you’re experiencing is normal, but you’re just not sure that’s true? This post is for you! Here are 10 signs that you should seek qualified breastfeeding help sooner than later.
For something that is supposed to be so “natural,” breastfeeding certainly doesn’t come naturally to most of us! Breastfeeding is actually a learned skill. And because of that, if you’ve never breastfed before, it can be really hard to know if breastfeeding is going well. That’s because most people who breastfeed will more than likely experience some initial awkwardness, frustration and discomfort as they learn something new.
Breastfeeding FACTS You Should Know
Our FREE guide will offers 12 breastfeeding secrets to help you avoid common issues.
What no one tells you about breastfeeding (but should)
This is what lactation consultants want you to know. Our FREE guide will give you 12 breastfeeding secrets that will help you avoid common problems.

Too often, breastfeeding parents are told that pretty much everything bad they are experiencing is “normal.” Extremely sore nipples? Normal. Uncomfortably full breasts? Normal. A baby who takes an hour to nurse? Normal.
Often, these things aren’t normal. Or, they can be normal in some circumstances, but are sometimes a sign of a problem that should be addressed. As a new-to-breastfeeding parent, how are you supposed to know where to draw that line?
Unfortunately, your child’s pediatrician more than likely won’t be much help here. Pediatricians are exceptionally knowledgable providers when it comes to childhood illness, growth, and development, but most do not have lactation training. And those who do may not be able to provide the support breastfeeding parents need in the 15-20 minute appointment time slot they have to work with.
This is where lactation consultants come in! A qualified and experienced lactation consultant has specialized training to support not only lactation, but pumping, bottle-feeding, and combo-feeding (feeding both infant formula and human milk) as well.
READ MORE: How To Find A Lactation Consultant Who Supports You
But still, you might be wondering: When should I see a lactation consultant?? Don’t worry! I got you. Here are 10 signs that you should get breastfeeding help right away:
RED FLAG #1: You are concerned breastfeeding isn’t going well, or might not go well in the future.
True breastfeeding issues rarely go away on their own and have a tendency to get worse over time. So any time you are concerned that breastfeeding isn’t going well, it’s best to get help as soon as possible. Even if you feel the worry might just be a small one! A “small” worry now could turn into a big concern later. Getting help early might save you from loads of frustration in the future.
If you’re not sure your concern warrants a full-blown appointment with an IBCLC (International Board Certified Lactation Consultant), consider joining a breastfeeding support group (I co-run this one–it’s free, online, and inclusive!) or attending a free in-person support meeting local to you. The peer counselor running the group can give you tips and let you know if your issue warrants professional attention. If you decide to meet with a lactation consultant, make sure they have the proper credentials and training to help with the issue you’re having (see this post for more info).

RED FLAG #2: Meconium is still present by the third day of life, or your milk has not increased in volume by 5 days postpartum.
When a baby takes in small volumes of milk after birth (yes, “colostrum” is milk!), their intestines push out stool for the first time. This early stool is called meconium. Meconium is thick, dark, sticky and tar-like, and it is made of cells, proteins, fats, and intestinal secretions that accumulated while baby was in utero.
Somewhere between baby’s 2nd and 5th day of life, your milk will increase in volume (i.e. “come in”). As baby consumes more milk, baby’s stool will begin to transition from dark meconium to a lighter yellow-gold (if breastfed) or tan (if formula-fed) color. Additionally, baby will stool more frequently as he or she ages. If baby is breastfeeding well, a normal newborn stooling pattering might look like:

If, however, baby’s stool is still very dark-colored by day 3, this is a sign that baby may not be breastfeeding well. Either way, your pediatrician should be notified. If your goal is to breastfeed, a lactation consultant (ideally an IBCLC) should evaluate baby’s latch and ability to transfer milk from the breast as soon as possible.
RED FLAG #3: Baby is not having enough wet and dirty diapers.
In the first four days of life, baby should have as many wet and dirty diapers as they are days old (e.g. 2 wets and 2 dirties on day 2, 3 of each on day 3, etc.). By day 5 through 6 weeks old, baby should have 5-6+ wet diapers and 3-4+ dirty diapers a day.
You might hear some parents say that it is “normal” for breastfed babies to go up to 7-10 days without stooling. Please note that this is NOT NORMAL for babies younger than 4-6 weeks! If baby is younger than 4-6 weeks old and is stooling less often than once a day, this can be a sign that baby is feeding poorly. After 6 weeks old, breastfed babies may stool less often than once a day, but wet diapers should still be plentiful and stooling should not be painful or difficult.
Always let your pediatrician know if baby is not having a sufficient number of wet and dirty diapers. But don’t stop there! A lactation consultant can help you figure out WHY this is happening (the cause is NOT always low milk supply!) and help you correct the underlying problem before things get worse.

RED FLAG #4: Baby loses more than 7-10% of his or her birth weight and/or is not back to birth weight by 2 weeks old.
It is normal for babies to lose some weight after birth, regardless of if they are breastfed or formula fed. During the first days of life, we monitor weight loss/gain and diaper output closely, since they give us an estimate of how well breastfed babies are feeding.
It is normal for breastfed babies to lose around 7% of their birth weight in the first several days of life. Although there is some evidence that losing around 10% of birth weight may not be unusual in some circumstances (one study found that >25% of newborns delivered by cesarean lost at least 10% of their birth weight), pediatricians start to get nervous–and rightfully so–when babies approach >7-10% weight loss. This can be a sign of feeding issues (although not always).
Slow weight gain in the first weeks of life is also a red flag for feeding issues that should be addressed immediately. If it takes longer than 2 weeks for a breastfed baby to get back to his or her birth weight, see an IBCLC right away. And if your pediatrician isn’t already aware, bring this to his or her attention.
READ MORE: How C-Sections & IV Fluids Affect Weight Loss in Breastfeeding Newborns
Important Note: Attending all well-check pediatrician appointments is very important, especially in the first weeks and early years of life. Pediatricians monitor weight gain, growth, and developmental milestones, and can identify health or developmental issues that the average parent does not have the training to recognize.
RED FLAG #5: Latch is extremely painful, or it is painful longer than 1-2 weeks
While some amount of nipple discomfort in the early days of breastfeeding is normal, significant pain is not. Excruciating pain at any time (and especially in the first 3-4 days of life) or pain that doesn’t go away by 1-2 weeks after birth should be addressed immediately. This is because nipple pain frequently indicates a latch issue. Left unchecked, latch issues can lead to slow weight gain in baby and milk supply problems (fortunately, both are treatable).
READ MORE: How To Heal Sore Nipples (The Right Way)

RED FLAG #6: You need to use a nipple shield to breastfeed
If you find you need to use a nipple shield to breastfeed, it would be a good idea to meet with an IBCLC. Nipple shields are not “bad” to use, and sometimes you only need to use one temporarily. That’s fine! But it is important to be aware that using a shield can sometimes mask underlying feeding issues. If baby cannot latch without a shield, if a shield must be used to prevent nipple pain, or if you’re having trouble weaning from a shield, I’d recommend seeing an IBCLC.
READ MORE: The Ultimate Guide To Nipple Shields (When & How to Use Them Correctly)

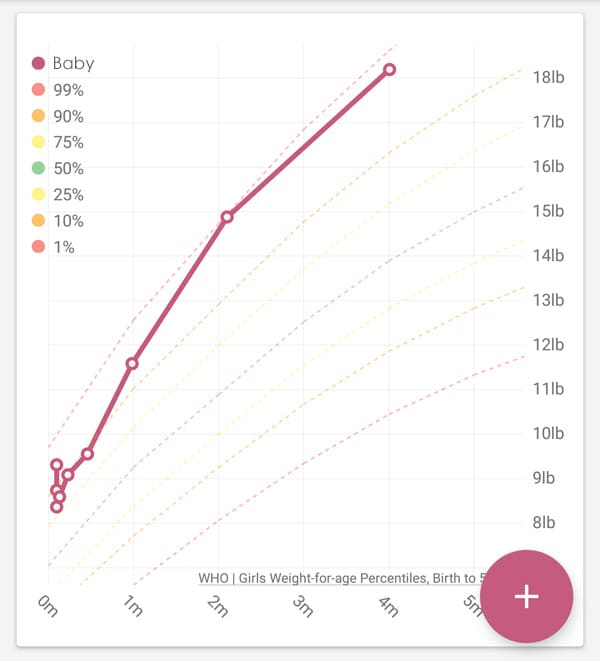
RED FLAG #7: Baby is gaining weight very slowly, or baby was gaining weight well but weight gain is noticeably slowing down (especially around 2-4 months old)
It is easy to disregard this red flag since baby is in fact gaining weight or gained weight well at one point. Too often, parents are told to try to make their milk “fattier” or to just supplement with formula. But these solutions don’t get to the root of the problem.
The body does not make low-fat milk, and you cannot increase the fat in your milk through diet changes. And while there is nothing wrong with formula use and supplementation is sometimes necessary, throwing bottles of formula into the mix doesn’t address any underlying problems.
Often, low milk supply is blamed for weight gain issues, but even that may have a root cause that needs addressing, such as poor latch or feeding habits that should be changed. Don’t wait to address these issues!

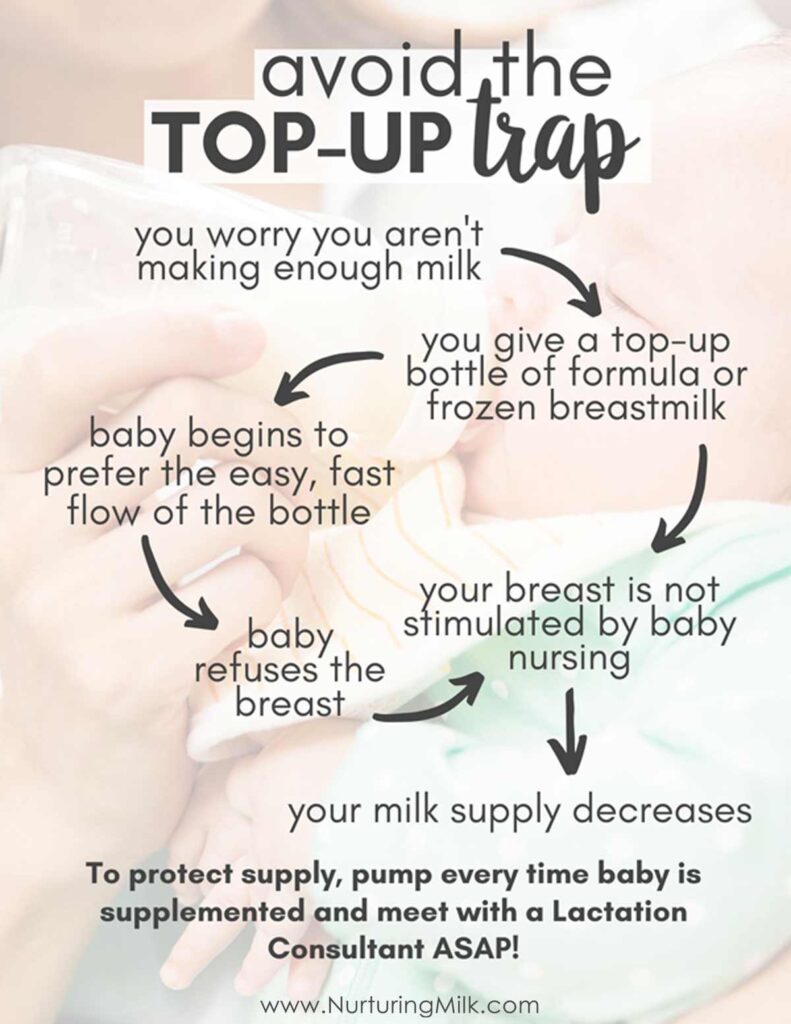
RED FLAG #8: Baby needs or is receiving supplementary bottles of formula or pumped milk.
Again, there is nothing wrong with choosing to supplement with formula. Combination feeding (offering breast milk and formula) works well for many families! But if your goal is to exclusively breastfeed, or if concern about your milk supply and/or baby’s ability to feed effectively is prompting you to supplement, it is a good idea to meet with an IBCLC and to protect your milk supply in the meantime (see note below).
Important Note: Feeding supplemental bottles of formula or frozen milk can lower your milk supply over time if steps are not taken to protect it. To protect your milk supply when supplementing, pump a full session every time baby gets a bottle of formula or frozen milk and make sure all bottles are pace fed.
READ MORE: Why I Don’t Recommend Lactation Cookies & Body Armor For Low Milk Supply
RED FLAG #9: Baby is less than 6 months old and your breasts are being drained less than 8 times in 24 hours, or you are following a parent-led feeding schedule.
Have you ever been told that by a certain age, a baby should be going at least X hours between feeds? Yeah, that’s a myth! And there is zero research to support the idea that babies’ feeds need to be spaced out as they age. This is actually a cultural norm that developed as more and more babies were fed by bottle in the 20th century. It is NOT reflective of how babies naturally eat, nor is it conducive to maintaining milk supply. Research has actually shown that parent-led feeding schedules (in which the parent chooses when and how often baby nurses) can cause low milk supply over time. And so can spacing out baby’s feeds! You can learn more about why this happens here.
Breastfed babies should always be fed on cue, especially as newborns. Babies tend to get hungry around the same times every day, so it is absolutely fine to feed according to baby’s natural feeding routine. To maintain milk supply, most breastfeeding parents will need to drain their breasts at least 8 times in 24 hours. A few may be able to nurse less often than this and maintain milk supply over time, but many will not.
If you are nursing fewer than 8 times in 24 hours and/or your feeding schedule is working well for you now, that’s great! You do not necessarily need to run to your nearest IBCLC or do anything differently. If things change, consider making adjustments to feeding frequency and meet with an IBCLC as needed.
Important Note: It’s normal and common for babies to “cluster feed” (i.e. have back-to-back nursing sessions) in the evenings and during growth spurts and developmental leaps. However, sometimes marathon nursing sessions (40-60+ minutes of nursing) can be a sign of a baby struggling to feed well. Bring this concern to an IBCLC.

RED FLAG #10: Your newborn is a very “good” baby (rarely cries, sleeps long stretches early on), especially if baby isn’t gaining weight well.
I saved this one for last because it is not super common, but it is still worth mentioning.
It might seem counterintuitive, but a “good” newborn can be a sign that baby isn’t feeding well. Most babies will protest when they are hungry, but some are happy to sleep through it. These babies may have a worried or anxious look on their faces when awake, may gain weight slowly, and/or may sleep long stretches overnight at an early age or fall asleep frequently at the breast. To be safe, it is a good idea to have these babies’ feeding behaviors evaluated by an IBCLC.
If baby is not receiving supplemental formula AND is showing good weight gain AND is having an appropriate number of wet and dirty diapers each day, baby is likely breastfeeding fine, but see an IBCLC and speak to your pediatrician if you are still concerned.

WANT TO PUMP MORE MILK? Try THIS!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
Want to pump more milk? try this!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
HUNGRY FOR MORE?
Check out my Breastfeed With Confidence online course. It’s focused on preventing the most common breastfeeding issues and helping you (re)build and protect your milk supply. Each lesson is only a few minutes long, accessible on mobile, and can be viewed at your own pace. It’s perfect for new parents AND those with prior breastfeeding experience! Here’s what one of my students had to say after taking it:
“I wish I would have had this class prior to my first child. I had numerous complications with breastfeeding my first baby, many of which I might have been able to prevent had I taken this course. I decided to take this course prior to having my second child, and was quite surprised how much more I learned, despite the numerous sessions with multiple lactation consultants I had with my first baby. Breastfeeding with my second child has been a much more enjoyable experience!”
You Might Also Enjoy:
- How To Find A Lactation Consultant Who Supports You
- Why I Don’t Recommend Lactation Cookies & Body Armor For Low Milk Supply
- Bad Breastfeeding Advice We Too Often Follow
- Is My Milk Drying Up? 10 Low Supply Myths You Need To Know
If you enjoyed this post, be sure to check out our digital library of helpful resources that quickly teach how to avoid common breastfeeding problems and give you the peace of mind and confidence you need to meet your breastfeeding goals.