Relactation: How To Bring Back Your Milk Supply
This post may contain affiliate links (see full disclosure). As an Amazon Associate, I earn from qualifying purchases.
Learn how to bring back your milk supply–even if you fully or partially switched to formula–with these relactation strategies. I discuss pumping tips, galactogogues (milk supply boosters), and what you should expect.
Parents switch to formula, either fully or partially, for a number of reasons—none of which require justification. Just because breastfeeding is “natural” doesn’t mean it’s always easy. And when breastfeeding doesn’t work out for whatever reason, commercially prepared infant formula is the healthiest and safest alternative to human milk. In recent decades, a LOT has been done to make modern formulas as close to breastmilk as possible. And science has allowed us to do a pretty darn good job of that!
WANT TO PUMP MORE MILK? Try THIS!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
Want to pump more milk? try this!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
But sometimes, parents who are fully or partially formula feeding wish to return to breastfeeding. This desire is often met with reassurance that “formula is just fine” and “fed is best.” While both statements are true, they may not help you. You may have compelling reasons to give breastfeeding a second chance anyway.

There are many reasons that a parent may wish to rebuild their milk supply (a.k.a. relactate). Here are a few that might resonate with you:
WHY BOTHER RELACTATING?
(If you’re already set on getting started with relactation, you can jump ahead by clicking here)
Formula isn’t agreeing with baby.
Infant formula, which is most often cow’s milk based, is unfortunately not tolerated well by all babies. For example, upwards of 15% of infants experience symptoms that suggest they are sensitive to cow’s milk proteins (source), and upwards of 7.5% of infants are affected by cow’s milk protein allergy (CMPA) (source). Fortunately, there are alternatives to standard cow’s milk-based infant formulas, including soy-, goat milk- and amino acid-based infant formulas. There are also hydrolyzed/extensively hydrolyzed formulas designed to be gentler on baby’s tummy.

However, the process of finding the right formula may take time and can prove stressful. Some babies may struggle during this process. Many babies sensitive to dairy are also sensitive to soy and goat’s milk. Sometimes “hypoallergenic” extensively hydrolyzed formulas will still bother baby. And many of these special formulas can be very expensive.
Some babies who don’t tolerate cow’s milk in infant formula have no problem consuming breastmilk, even if the breastfeeding parent is consuming dairy. Other babies need their breastfeeding parent to follow a dairy-free (or other allergen-free) diet in order to feed safely. When infant formula isn’t agreeing with baby, relactation may be a viable alternative.
READ MORE: Dairy Intolerance in Breastfed Babies (What You Can Do About It)
Unmet Desires and Breastfeeding Grief
Some parents who wish to relactate feel grief or disappointment that their breastfeeding journey didn’t go the way they hoped it would. Relactation can be an opportunity for a “do-over,” a second chance at fulfilling an unmet personal desire.
Some parents find that they just miss the feelings of closeness breastfeeding can provide. While it is absolutely the case that parents of bottle-fed babies are able to bond with their infants, some parents feel that the bond they had while breastfeeding was unique, and they want to experience that again.

Other parents may feel they turned to formula prematurely. This can prompt feelings of grief or guilt, even though there is nothing wrong with using formula and even when no one is blaming them for needing or choosing it. Many breastfeeding parents reduce or lose their milk supply accidentally, not realizing that offering supplemental bottles of formula or previously frozen breastmilk can result in low supply over time. Many parents are incorrectly told they must wean in order to take medications that are actually compatible with breastfeeding. And many parents are given poor (or no) breastfeeding support, causing them to turn to formula when they may not have otherwise needed to. When a parent feels circumstances robbed them of a desired breastfeeding experience, relactation—or even just attempting it—can sometimes offer healing.
Breastfeeding offers the type of flexibility you seek.
Let’s be honest: Breastfeeding can be exhausting and time consuming. Especially in the first few weeks postpartum, when it might seem like baby is on the breast more often than not! Furthermore, many new breastfeeding parents worry about their ability to feed baby in public, making it difficult to get out of the house. For these reasons (and many others), breastfeeding can feel mentally taxing. Offering a bottle of formula or previously frozen milk can help alleviate much of this burden.
After a while though, some parents find that bottle-feeding no longer offers them the flexibility they seek. It takes time to prepare formula properly, wait for milk to cool, and wash bottles. It also takes time (and usually two arms, if you’re bottle-feeding appropriately) to feed a bottle. And if you go somewhere, you must plan to carry enough milk with you for however long you’ll be gone.

In contrast, many parents find that over time (especially after the first month), breastfeeding gradually becomes easier and more efficient than it once was. There are no bottles to prepare and nothing that needs washing or sterilizing. You can breastfeed lying down with your eyes closed at 2am, and breasts are very portable (and hard to forget at home). If your baby was able to feed at the breast before, being able to do so again might make relactation an appealing option. (Even if your baby has never fed at the breast, it’s possible he or she may be able to learn how!)
REALISTIC EXPECTATIONS
Before you begin pumping up a storm trying to bring your supply back, it’s important to recognize that relactation is a process, and one that doesn’t happen overnight. It will take time and commitment.
In fact, it will possibly take a lot of time: The longer it has been since you produced milk, the longer the process of relactation may take. Around 40 days after your last breastfeeding session, the cells that produce milk in the breast begin to die off (a gradual process called “involution”). So if it has only been a couple weeks since you last breastfed, those milk-making cells are largely intact, and you may find it only takes a couple weeks of consistency to rebuild your milk supply. If it has been 40 days or longer since you last breastfed, more of those milk-making cells will have died off. But this doesn’t mean all hope is lost! It just means it will take longer to regrow these milk-making cells and get them producing.

Regardless of how long it’s been since you last breastfed, relactation requires committing frequently pumping throughout the day. It is normal for someone rebuilding their milk supply to need to double-pump for 15-20 minutes at least 8 times in 24 hours, with at least one of those sessions happening overnight. At times, you may find yourself feeling like you are taking two steps forward and one step back. You may find yourself making what appears like no progress for weeks before you notice improvement. This is normal. No two relactation journeys are the same.
What if you’re on the fence?
If you’re not sure you’re up for this commitment, that’s okay! Having these realistic expectations will at least help you make an informed decision. Some parents decide to commit to building their supply over a certain timeframe (e.g. X days or weeks) before deciding if they will continue, so you don’t have to fully commit right away. In the end, the amount of time and effort involved in relactation may not be worth it for your family, and there’s nothing wrong with that. It’s a personal decision, one that only you can make for yourself.
If you’re still committed to relactation but are feeling discouraged or impatient at the prospect of it requiring so much time, keep in mind that even if it takes a while to establish a full milk supply, you may find you get decent-sized volumes to supplement with in the meantime. Some breastfeeding parents find that this is sufficient to meet their goals and offer formula or donor milk to make up the difference. That’s okay too.
Finally, it’s also good to note that relactation will probably require some tools. While it is technically possible to bring back milk supply without using a breast pump, it is usually much quicker and easier to use one. We’ll talk about this more below.
THE IMPORTANCE OF SUPPORT
Before we start talking about the steps involved in relactation, it’s important to emphasize that good breastfeeding support can be a critical part of this process. If you can, it might be a good idea to meet with an IBCLC (International Board Certified Lactation Consultant) prior to starting. A qualified IBCLC can help you address any issues that may have interfered with your breastfeeding journey the first time around (e.g. low milk supply concerns, etc.) and may be able to help you avoid those issues (and others) this time. In addition to being able to help with things like breast pump settings and flange fitting, an IBCLC is also equipped to support getting baby to latch and breastfeed (if that is something you would like to do) once your milk supply has increased in volume, so it may be good to meet with one as needed throughout the process.
The breastfeeding support you seek during this process does not necessarily have to be exclusively professional support. There are facebook groups and peer support organizations, such as Breastfeeding USA and La Leche League, where you can get free support and encouragement from breastfeeding parents and peer counselors who have been in your shoes. At the very minimum, I highly encourage you to seek this free support online, in-person, or both.
For more information on how to find a qualified lactation consultant in your area, be sure to check out this post. Again, good breastfeeding support can be a hugely important part of the relactation process (I cannot emphasize that enough). Not all lactation consultants or support groups are created equal, so don’t be afraid to shop around or look for new support if what you found first isn’t helping.
Medical Disclaimer: The content of this blog post is not medical advice nor is it a substitute for medical advice, diagnosis, treatment, or professional lactation care. This post is for educational and informational purposes only. It is the reader’s responsibility to review all information regarding any medical condition or treatment with a healthcare provider.
REBUILDING YOUR MILK SUPPLY: HOW TO GET STARTED
Note: There are three ways the breast can be stimulated to produce milk: By a baby, by hand, or by a pump. During relactation, most parents rely on pumping to stimulate the breasts, since baby may not be willing or able to breastfeed, especially if little to no milk is available. While it is technically possible to relactate with hand expression alone, pumping is usually faster, easier and more effective. For the purposes of this post, I’ll assume you’ll be primarily pumping to rebuild your supply. However, a baby who is willing to latch and suckle can eventually help rebuild supply as well.
Every time the nipples are stimulated and milk is removed from the breast, your body gets a signal to produce more milk. And frequent removal of milk speeds up milk production over time.
Think of it like a diner: Expressing milk is like a waiter putting in an order so that the kitchen knows it needs to make a plate of food. If no one has been to the diner in a long time, the kitchen staff will need some time to stock up on ingredients and get the kitchen ready to serve customers. During this time, you probably won’t be able to express much (or any) milk, but it’s still important to keep “putting in the order” (i.e. pumping) so that your “kitchen staff” knows there are customers waiting (so to speak). Eventually, you’ll put in an order and the kitchen staff will make some food. If you put in a lot of orders, over time the kitchen staff will become efficient at making a lot of food.

If your diner only gets a few “orders,” it will only make a bit of food. Likewise, if you consistently miss or skip a pumping session, your milk supply will start to reflect that. So it’s important to send those “make milk!” signals to your breasts often by pumping frequently, even if pumping doesn’t yield milk at first.
HOW OFTEN SHOULD YOU PUMP?
The hormone responsible for the “make milk!” signal is called prolactin. Prolactin levels double when the breasts are stimulated, and they peak about 45 minutes after the beginning of a breastfeeding or pumping session. We want to elevate prolactin levels as often as possible. The best way to do this is to use a breast pump to mimic how often a newborn breastfeeds, which is usually 8-10 times (or more) in 24 hours. If you pump at least 8 or more times in 24 hours, prolactin levels won’t decline completely before they rise again at the next pumping session. Since we want to keep prolactin levels elevated, aim to go no more than 2-3 hours between pumping sessions during the day and no more than 6 hours between pumping sessions at night.
Speaking of night-time: Ideally, at least one of your pumping sessions should happen overnight, between 1am and 3am. This is so you can take advantage of the fact that prolactin levels are highest during this time, and because long stretches between pumping (or nursing) sessions sends a signal to your body to slow down milk production. That said, most lactation professionals agree that one longer stretch of no more than 6 hours overnight is fine.
According to Lucy Ruddle, IBCLC (who wrote an excellent book on this topic that I encourage you to read), a sample pumping schedule might look like: 6am, 8am, 10am, 12pm, 3pm, 6pm, 9pm, 3am. Or you could try something like 6am, 9am, 11am, 2pm, 5pm, 7pm, 10pm, 1am.
Note: If you can tolerate pumping closer to 9 or 10 times in 24 hours, this may help. However, pumping this much may not be necessary, and if pumping that often is too much for you, rest assured that 8 times in 24 hours is sufficient for many relactating parents. Your mental health matters too!

PUMPING TIPS
Selecting a Pump and Getting Started
When you pump, be sure to express milk from each breast for at least 15-20 minutes. A double electric breast pump allows you to pump both breasts at the same time, but a single electric breast pump or a hand pump can also work if necessary. Before pumping, consider spending a few minutes gently massaging the breasts and/or applying warm compresses. This is a great way to “warm up” the breasts and encourage milk flow, but it doesn’t need to take more than a couple minutes.
When using your pump, you will need to make sure that it has a strong motor in good working order (older or used pumps may have worn out motors). Some parents may opt to rent a hospital-grade pump (these have durable motors and are designed to be safely used by more than one person). If you’re in the U.S., check with your insurance provider to see if you are eligible to get a pump covered by insurance. The two regular breast pumps that, in my experience, parents tend to prefer are the Spectra pump (S1 or S2) and the Medela pump. Between these two, parents generally tend to prefer the Spectra a bit more. If you are in the market for a new breast pump, ask your local IBCLC or breastfeeding groups which pumps they recommend. There are many more options than just the two I mentioned here!
A hands-free pumping bra or pump flanges that allow you to pump discreetly (such as Freemie cups), might also be worth looking into. These allow you to (as the name would suggest) be hands-free while pumping. They also make wearable breast pumps (such as the Willow or Elvie pump) that allow you to pump on the go! However, wearable pumps tend to be hit or miss in terms of how well they work for some people, and they can be expensive. Also, hands-free pumping setups don’t allow for hands-on pumping.
Hands-On Pumping
Hands-on pumping is a technique that involves hand massaging the breasts while you pump. It’s not strictly necessary to use this technique, but research has shown that it can help you pump more milk. Milk expressed this way also often has a greater fat content (i.e. more calories), since manually compressing the breast pushes more fat through the ducts.

To try hands-on pumping, make a C shape with your hand, placing your thumb on top of the breast and the rest of your fingers below it. Then gently compress the breast, using the palm of your hand to apply gentle but firm pressure as well. Be sure to keep your hands closer to the wall of your chest and away from the pump flange so you don’t accidentally knock it and lose suction! After a few compressions, rotate your hand a bit (as though you were moving around a clock face) and compress again.
Selecting The Right Flange Size
When using your pump, it is critical that you are using the correct flange (a.k.a. “breast shield”) size. This is the piece that sits directly on top of your breast while you’re pumping. Most pumps come with a standard 24mm flange, but this size doesn’t fit everyone. If the flange is too big or too small, you won’t be able to pump as much milk! The wrong flange size can also lead to nipple pain and discomfort. You want the flange to be large enough for your nipple to move freely, but not so large that too much of the areola is pulled in.
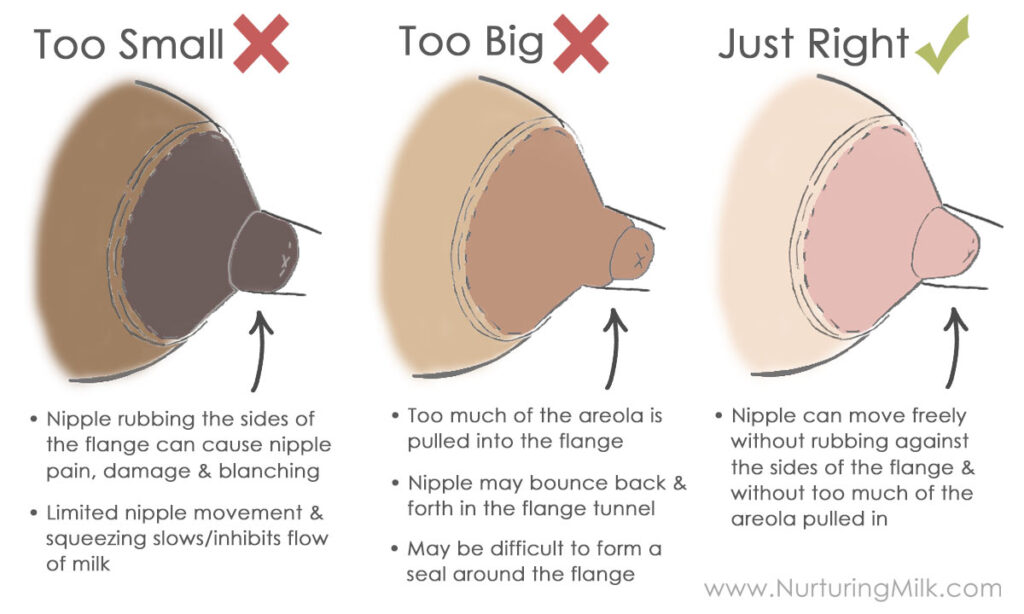
For more information on how to determine if the flange size you’re using is the best fit for you, read this post. If you’re still having trouble sizing your flanges, an IBCLC or breastfeeding counselor can help! If you find that your nipples are pretty stretchy (“elastic”) and get pulled far into flange, you may benefit from a flange insert (such as Pumpin’ Pals, Maymom inserts, or BeauGen inserts) to help prevent this.
Selecting The Right Pump Settings
An electric breast pump will let you adjust motor speed and suction strength. While it may be tempting to turn the pump all the way up and go to town, this won’t give you the best results! Instead, we want our pump settings to mimic what a baby would do at the breast.
When a baby nurses, they start out with a few minutes of lighter, faster sucks. This type of sucking stimulates nerves in the breast to send a signal to the brain. The brain in turn releases a hormone that allows milk to start flowing from the breast. This is called the let-down reflex. Once milk starts to flow, baby’s sucks become longer and deeper. This is the sucking pattern we want to mimic with our pump settings.

To figure out how high your pump suction should be, turn your pump on and slowly turn the suction up to the highest setting that feels comfortable. When you begin pumping, your suction will be a bit less than this, and the cycle speed (the speed of the motor) will be faster. Once milk starts to flow (or after about two minutes if your supply isn’t there yet), turn the suction back up to that comfortably high setting, and slow down the cycle speed. Some pumps, such as the Medela PISA, have a built-in setting where all you need to do is adjust the suction strength: The pump will automatically begin with an increased cycle speed for 2 minutes before switching to a slower cycle speed after that time.
If you need help adjusting your pump settings, a lactation consultant, breastfeeding counselor, or peer supporter may be able to assist you. There are also loads of good videos online to help you adjust settings on just about every pump available.
Power Pumping
Some pumping parents swear by power pumping as a way to boost milk supply. Power pumping isn’t strictly necessary, but it is a tool at your disposal that will help you mimic newborn cluster feeding. This frequent feeding over a relatively short period of time helps encourage increased milk production. To power pump, begin by pumping for 15-20 minutes before taking a 10 minute break. Then begin pumping for 10 minutes and take another 10 minute break when you’ve finished. Pump for 10 more minutes, and then you’re done!

Hand-Expression
Hand expression can be a useful way to express milk early on in your relactation journey (when you aren’t producing much and drops can get lost in the crevices of your flange) or at the end of a pumping session (when you may be able to express a bit of extra milk by hand). If hand expression proves effective, it may be tempting to rely on hand expression exclusively. Indeed, some have done this! But it’s not easy, and a breast pump may still be more effective/efficient for you in the long run. To learn how to hand express, see this post here.

Realistic Pump Output
It’s important to have realistic expectations about what normal pump output looks like any time you pump—relactating or not. Normal pump output in a person with a full milk supply is only about 2-4 ounces both breasts combined when you’re pumping for a missed feed! It’s also normal to be able to pump more milk in the morning than you can at night (milk produced in the morning has a higher water content, giving it more volume, while milk produced in the evening is a bit more nutrient-dense due to a lower water content), and it’s normal for one breast to pump more than the other (you don’t need to do anything to fix this).

Remember that it can be normal to pump little to no milk in the beginning of your relactation journey, and there is no reliable way to predict when you will start to see increased milk volumes. If you find yourself concerned that you aren’t progressing, reach out to a qualified IBCLC and/or support group for help and encouragement.
READ MORE: How Much Milk Should You Pump? (What’s Normal and What’s Not)
MILK BOOSTING FOODS, DRINKS, HERBS AND PHARMACEUTICALS?
Any time a breastfeeding parent asks online about how to increase milk supply, one of the first suggestions given is almost always some kind of milk boosting supplement. Herbal capsules, lactation cookies, mother’s milk teas, sports drinks, oats, gallons of extra water—all of these are commonly recommended. But do they work?
Maybe, maybe not. The truth is, there isn’t a lot of quality research on the efficacy of these milk boosting products (a.k.a. galactagogues), and what research there is doesn’t strongly suggest that they actually work (source). Some researchers suspect a placebo effect: It could be that consuming something you believe will increase your milk supply helps you relax enough to pump more milk (after all, stress can inhibit your letdown).

If you do decide to try a galactagogue, just don’t let it distract you from frequent pumping. Many non-herbal foods traditionally thought to be supportive of a strong milk supply (like oats, garlic, barley, etc.) tend to be healthy, whole foods that should probably be a part of our diets anyway. They are unlikely to hurt you, and if you find that they help, then that’s great! Just remember that nothing you can consume to increase milk supply will help significantly if you’re not also pumping often enough.
Furthermore, it’s important to remember that glactogogues are not a substitute for professional lactation care or breastfeeding support. It can be tempting to delay seeking help and instead wait to see if the galactagogue you’re taking will fix the problem. Don’t delay!
Lastly, before you take an herbal galactagogue, always speak with your healthcare provider. Just because a product is “natural” doesn’t mean it is always safe. Natural products can interact with certain medications or affect certain medical conditions, and they can also cause problems if taken in excess.
Here are a few more things about galatcagogues you should be aware of:
READ MORE: Why I Don’t Recommend Lactation Cookies & Body Armor For Low Milk Supply
How much should you take?
Because there is very little quality research on the efficacy and safety of many galactogogues, we don’t know a lot about how much one should consume in order to see results. It is possible that the $21 lactation cookies you’re considering may contain too little galactagogue to have a significant impact. The book Making More Milk offers a pretty thorough review of galactoguges, including dosing suggestions, if you decide to give them a try. Again, always consult your physician before starting.
Fenugreek
Fenugreek is an ingredient often found in lactation cookies and mother’s milk teas. But this ingredient is known to sometimes cause upset stomach and gas in breastfeeding parents and their babies, and it’s not recommended for people with diabetes, hypoglycemia, hypothyroidism, asthma, people with blood clotting or bleeding disorders or who are on medications to slow blood-clotting, and people who are allergic to peanuts or chickpeas (source). You should also be wary of NSAIDs if you’re taking fenugreek. Anecdotally, some breastfeeding parents report fenugreek lowering their milk supply rather than boosting it.
Milk Thistle
Milk thistle is a commonly used galactagogue that has some evidence supporting its use, although it is weak. Milk thistle should be avoided if you’re allergic to ragweed, common thistle, daisies, artichokes or kiwi. Use milk thistle with caution if you are taking anti-seizure medications, antipsychotic drugs, antianxiety drugs, oral diabetes medications, or blood thinners. Milk thistle may also make hormonal birth control pills less effective (source, source, source).
Beer/Alcohol
Many breastfeeding parents are told to drink beer to increase their milk supply. While alcohol consumption in moderation while lactating is generally considered safe, it’s important to note that alcohol can actually interfere with your letdown, resulting in a lowered pump output. It’s more likely that any reported positive effects from beer came from the barley and hops, not the alcohol.

Gatorade, Body Armor, and Coconut Water
Anecdotally, parents report these drinks boost milk supply, but there isn’t research to support this. These drinks do have potassium, which can be helpful if you are dehydrated. However, these drinks also tend to contain a lot of sugar and empty calories. You can just as easily meet your potassium needs through diet and your hydration needs through water.
“Drink lots of water”
It is safe and sufficient to simply drink to thirst when breastfeeding. Drinking extra water beyond this does not result in increased milk production (source, source).
Domperidone/Metoclopramide (Reglan/Maxeran)
These are two pharmaceutical drugs intended to treat conditions of the GI tract. However, they are used “off-label” to increase prolactin levels, since that is a known side effect of both. If you do not have low prolactin levels or other underlying issues, it’s possible these drugs may do little for you.
In the U.S., Domperidone is no longer an approved drug after epidemiological reports linked its use to serious cardiac arrhythmias, especially in elderly patients. It is technically not approved in any country for use in breastfeeding parents; however, it is prescribed off-label to parents in other countries such as Canada, Australia, and the UK. Since it can interact with other drugs/conditions, Domperidone should only be used under the guidance of a healthcare professional. Long-term use of Domperidone may bot be advisable, and weaning from it should be done gradually to avoid withdrawal side effects (source).
Metoclopramide (Reglan/Maxeran) is available in the U.S., although it is known to cause side-effects such as restlessness, drowsiness, fatigue, irritability, depression, racing heart, and involuntary body movements, especially if you’ve been using it longer than 2-4 weeks. Metocopramide should probably not be taken if you have a history of depression or if you are on SSRIs or anti-depressants. In general, this drug is roughly 4x more likely to cause side effects compared to Domperidone (source).
PUTTING BABY TO BREAST
If your eventual goal is to have baby feed from the breast, you can practice getting baby comfortable there with frequent skin-to-skin contact. This involves stripping baby down to just a diaper, reclining, and putting baby belly to belly on your bare chest/stomach. Skin-to-skin contact is useful because it helps stimulate baby’s innate feeding reflexes. The goal with skin-to-skin time–at least at first–is to make the breast a safe, warm, and inviting place to be. If baby doesn’t seem to like skin-to-skin time, don’t force it! Instead, introduce it slowly and gradually.

If it hasn’t been too long since you last breastfed, you may find that baby naturally seeks out the breast and starts latching during skin-to-skin time. If so, that’s great! You can start offering the breast more often as you continue to build up your milk supply. Over time, as baby takes more from you directly, you can begin to reduce the amount of supplemental feeds (pumped milk or formula) baby receives. This should be done carefully and gradually, so you don’t accidentally or prematurely reduce pumping/your milk supply before it is where it should be. The book Relactation: A Guide To Rebuilding Your Milk Supply offers many more in-depth suggestions and guidance for transitioning to at-breast feeding. An IBCLC would also be an invaluable resource at this point.
If your baby isn’t able or willing to latch, or if you’re not sure that baby has an effective latch (perhaps it is painful or baby seems frustrated at the breast), I cannot emphasize enough how important it is to get qualified breastfeeding support. Again, you can check out this post for more information on where to find good support. And if you’re still having trouble, feel free to contact me! I will do my best to help you find someone in your area.
IS MY BABY GETTING ENOUGH?
It is very common for relactating parents (especially those who have a history of breastfeeding troubles or low milk supply) to be wonder if baby is getting enough milk, especially as they begin to transition to at-breast feeding. Speaking with a lactation consultant about your concerns can help ease your mind.
If you’ve begun to transition to at-breast feeding, remember that we would expect your pump output to decrease a bit, as baby is now getting some milk from you directly. If you’re noticing this, it may be normal.
If you are bottle-feeding expressed milk and your baby doesn’t seem satisfied, the problem may be in how bottles are being fed. Keep in mind that breastfed babies consume 25-30 ounces (750-900ml) per day on average, but it is common for babies who are NOT pace fed to consume much more milk than they require. I’ve seen some babies given much as 50oz a day! This can put unnecessary stress on you to pump more milk than your baby actually needs. Babies should always be pace-fed bottles to help prevent accidental overfeeding (which is actually quite easy to do and quite common).

Lastly, keep an eye on your baby’s diaper output and weight gain. Baby should be having an appropriate number of wet and dirty diapers. That usually means 6 or more heavy, wet diapers with light colored urine (occasionally 5 heavy wet diapers is acceptable) and roughly 1 dirty diaper a day (although stooling frequency varies widely among babies, with some stooling only once every few days). Be on the lookout for changes in your baby’s voiding and stooling patterns and report them to your lactation consultant and pediatrician if you have concerns. A lactation consultant or your pediatrician can assist with keeping track of baby’s weight on an infant scale once every 2 weeks or so, if needed.
MORE RESOURCES
There are many more rabbit holes I could venture down on the topic of relactation, but this post is already quite long! If you’d like more information and resources, however, here are a couple books you may find quite useful during this process (click or tap the images below to see these books on Amazon):
I also recommend this facebook group, which has many IBCLCs and relactating parents ready and waiting to support you! If you’re interested in general breastfeeding support, you might also enjoy this non-judgmental, formula-friendly group I co-run.
Congratulations on making it to the end of this post (it was a long one!!), and best of luck to you as you move forward.
WANT TO PUMP MORE MILK? Try THIS!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
Want to pump more milk? try this!
Our FREE guide will give you 5 simple, proven tips to boost your milk supply and increase your pump output (no lactation cookies needed).
You Might Also Enjoy:
- Does Your Breast Pump Flange Fit Well? (Rethinking How To Size Flanges For Best Fit)
- How Much Milk Should You Be Pumping? (What’s Normal & What’s Not)
- How Much Milk Should You Be Pumping? (What’s Normal & What’s Not)
If you enjoyed this post, be sure to check out our digital library of helpful resources that quickly teach how to avoid common breastfeeding problems and give you the peace of mind and confidence you need to meet your breastfeeding goals.